Nonprofits tasked with shoring up the country’s supply of donated organs for transplant are overwhelmingly underperforming at their job, according to federal data released Friday, contributing to a national organ shortage.
The data from the Centers for Medicare and Medicaid Services (CMS) is part of new standards for measuring performance meant to improve accountability in an industry laden with problems. It shows falling performance scores for the nonprofits, known as “organ procurement organizations,” based on the number of organ donors and resulting transplants compared with how many donors were possible. For 2021, just 15 of the nation’s 56 organizations were in the top-performing tier, a decline of five from the prior rankings. Another 18 were in the second tier—up by two—and must compete for their contracts during the next contract cycle. And 24, two more than in 2020, were in the lowest tier—some 42 percent of all organ procurement organizations.
42%
of organ procurement organizations were ranked in the lowest performing tier in 2021
Such performance problems aren’t new, but until 2021, the nonprofits self-reported their results to regulators, making it impossible to compare them apples to apples. Agency oversight has ignored crucial parts of the delicate work of persuading families to donate their dying loved ones’ organs. It’s part of a track record of chronic opacity that has drawn congressional scrutiny and that experts and auditors say has contributed to the industry falling short by thousands of donations each year, up to 28,000 organs annually according to some advocates. Despite this, no organ procurement organization has lost its multimillion-dollar contract with CMS because of poor performance.
The new performance standards use an external measure of how many donors were possible instead of having the procurement organizations self-report this. Because the measures have improved, a potential crackdown is looming: Organ procurement organizations that do not meet the new standards by 2024 are slated to either lose their contracts—if they’re found to be in the lowest performance tier—or compete to maintain them when that data is used in the 2026 recertification period.
Even as they tighten performance reporting, though, regulators largely overlook a crucial part of the organ donation process: how exactly organ procurement organizations do their jobs. Documents obtained by The Markup and interviews with industry veterans show vast differences in performance standards, poor federal monitoring, and shortfalls in training. Regulators, for example, do not evaluate the procurement organizations on how often they show up to hospitals when called about a possible donor, how well they interact with families of the dying, or why they choose not to pursue someone for donation.
Critics say CMS and other regulators should be more closely monitoring the nonprofits’ operations.
“We are standing around in a dark room with a light switch,” said Brianna Doby, a health services researcher who previously consulted for organ procurement organizations.

Organ Failure
Poorer States Suffer Under New Organ Donation Rules, As Livers Go to Waste
Life-saving liver transplants have plummeted in some Southern and Midwestern states with higher death rates from liver disease, while New York and California have made big gains
The organizations’ main trade group, the Association of Organ Procurement Organizations (AOPO), said the CMS measure is adequate for measuring performance. “The ultimate measure of the authorization process is whether an organ was donated and successfully transplanted, which is captured in the CMS metrics,” said Barry Massa, president of AOPO.
CMS’s chief medical officer, Lee Fleisher, said CMS has requirements for how organ procurement organizations do their jobs as a condition for receiving payments from Medicare and Medicaid. But in the regulations it pointed The Markup to, many of the requirements included having established processes but not what the processes should be.
Organ procurement organizations’ performance has long been a contentious subject, as performance varies widely across the close-knit industry. The new grading system from federal regulators is meant to address this; it measures how many donors each procurement organization had in a given year and how many transplants resulted, compared to a deaths metric provided by the Centers for Disease Control and Prevention for how many donors were possible. The data lags by about two years. AOPO sent an April 18 letter to Sen. Ron Wyden (D-Oregon) expressing concern over the large number of procurement organizations that would be decertified and the lack of a publicized process for how competition and decertification would work.
Poor performance among the organizations has dogged the organ donation pipeline for years. One organ procurement organization, LiveOnNY, did such a poor job that its contract was nearly taken away twice. LiveOnNY’s chronically weak performance set the stage for hospitals in the area to form a lobbying group with hospitals in Massachusetts and a procurement organization in Los Angeles. The group recruited patients for a lawsuit that would allowed hospitals nationwide to obtain organs from a larger geographic area. (In an investigation published last month by The Markup and The Washington Post, we found that the new policy is itself riddled with problems and was orchestrated by a small group of executives, including organ procurement organization leaders.)
The Markup obtained a 2019 audit of LiveOnNY’s performance as part of that investigation and is publishing it below.
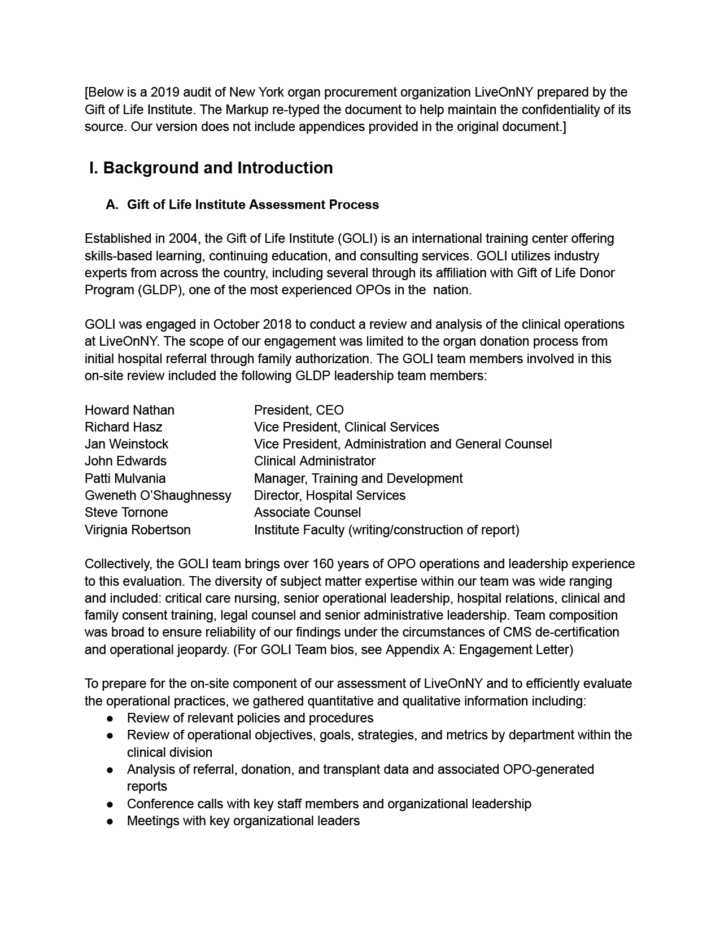
LiveOnNY ranked in the lowest-performing tier for the most recent rankings.
Who Gets to Donate
The differences in how organ procurement organizations do their jobs begin long before their staff set foot in a hospital. Under federal law, hospitals must alert their local organ procurement organization to any potential candidate for organ donation. But it’s up to each nonprofit to decide, in consultation with the hospitals they serve, how to determine at what point a hospital should alert them. Federal regulations do not spell this out.
These “clinical triggers” vary greatly. Organ procurement organizations and hospitals do not always publicize their triggers, but The Markup reviewed more than a dozen it found publicly posted or obtained from other sources.
Loss of brainstem reflexes, such as whether someone’s pupils react to light, is a common requirement because it is used in diagnosing brain death—but how many of those reflexes must be lost depends on the nonprofit. Some require just one reflex to be absent, while others require two. Many use a scoring system for brain functionality called the Glasgow Coma Scale that gives patients points based on their eye, verbal, and motor responses, but organ procurement organizations differ on what that score must be before hospitals alert them. Some don’t use this scoring system at all.
Requirements also vary on how quickly hospitals must inform organ procurement organizations about a potential donor. Many organizations require hospitals to call within an hour of someone meeting criteria for possible donation. Others let hospitals wait up to four hours. Waiting too long can mean a patient could die in a way that makes their organs unsuitable for donation.
There’s no research tied to it. It’s all observational.
Ginny McBride, OurLegacy, speaking of clinical triggers for best donation outcomes
The organ procurement organizations are also responsible for communicating these standards clearly to the hospitals they work with, something that does not always happen. In the assessment of LiveOnNY that The Markup obtained, auditors found that “basic information about standards of practice or clinical triggers were requested but not made available” by LiveOnNY to hospital leaders.
LiveOnNY did not respond to requests for comment.
Unlike nearly all other areas of medicine, which clinical triggers produce the best donation outcomes isn’t rooted in years of evidence-based practice, according to people involved with organ procurement organizations.
“There’s no research tied to it,” said Ginny McBride, CEO of Florida-based organ procurement organization OurLegacy. “It’s all observational.”
OurLegacy ranked in the top performance tier in the most recent data.
Staffing
Whether a terminally ill or injured patient becomes an organ donor depends on the nature of their condition, but it also hinges on how staff at organ procurement organizations perform their duties.
At the most basic level, staff need to quickly travel to hospitals in order to assess whether someone could be a donor and talk with that person’s family about the best course of action if they want to pursue donation. Not all organ procurement organizations have a good track record on this. The LiveOnNY audit, for example, found that LiveOnNY staff routinely failed to show up at hospitals when called.
CMS does not assess why an organ procurement organization did not approach someone for donation.
Among the most challenging parts of the job is talking with dying patients’ families. While CMS requires “discretion and sensitivity” for families’ beliefs around donation, the agency does not measure these crucial soft skills. And it’s up to each organ procurement organization to train its staff for these interactions. Some have specialized teams for this and other aspects of the donation process, while others have employees trained in a broader set of skills.
LiveOnNY staff, for example, weren’t uniformly trained, auditors wrote in 2019, and many were so specialized it complicated the donation process. The audit also found that much of the training was done on the job and did not include “competency checks particularly as it relates to communication skills.”
Staff in charge of getting authorization from families would delay approaching families because they were concerned about being denied, which “has certainly resulted in lost donation opportunities,” the audit found.

There aren’t uniform requirements for degrees or training required to perform such work. Employees can obtain a Certified Procurement Transplant Coordinator certification, but this is voluntary in the industry and not required by all nonprofits. To help fill this gap, one university, the University of Toledo, offers a master’s degree in transplantation and donation sciences. The university offers both an in-person track for those looking to break into the field and an online track for those currently in the field looking to improve their skills in a particular area.
What sets its training apart is standardization and training across the entire organ donation process, as opposed to specializing in a particular aspect such as approaching the family, Julie DeSantis, the university’s program director for transplant and donation sciences, said. Its graduates have been employed at dozens of organ procurement organizations across the country, according to its website. The transplantation program’s graduating classes are small, however—10 at most.
Regulation
To better measure the nonprofits’ performance, regulators would need to look at organ procurement organizations’ processes, not just their outcomes, some people close to the system said.
“If we think the process is tightly connected to the outcome, figuring out where [there] are breakdowns in the procedure can help you improve the number of organs that are recovered,” Benjamin McMichael, health law professor at the University of Alabama, said.
Some of this data is already in the hands of those that oversee organ procurement organizations.
The United Network for Organ Sharing (UNOS) is the nonprofit that operates the federal transplant system under a federal contract. It has operated this system—the Organ Procurement and Transplantation Network—for nearly four decades. As part of its duties, it oversees organ procurement organizations. Nadine Hoffman, UNOS director of enterprise data management, said that UNOS does not have the power to “impose sanctions, including payment and decertification,” as CMS does.
The procurement organizations are required to submit a form for every death that could have become a donation and for each “imminent neurological” death. The form, called the “death notification registration,” contains demographic information about the patient, when they were referred for donation, if they ended up donating, whether consent was obtained by the family, cause of death, and how they died, among other factors. This information could allow regulators to identify patterns in who isn’t pursued for donation and identify areas for improvement.
UNOS does not use the information in this form to evaluate organ procurement organizations’ performance, Hoffman said. It shares the data collected through the form with the Health Resources and Services Administration, the branch of the U.S. Department of Health and Human Services that directly contracts with UNOS. Hoffman said that UNOS is “discussing whether it would be beneficial” for it to collect “different information—particularly now that CMS has established new metrics for determining [organ procurement organization] performance.” She did not elaborate on what information that might be.
CMS does not receive data collected through the form, according to Fleisher, the agency’s chief medical officer. Instead the agency conducts its own surveys every four years to recertify the organ procurement organizations, mandating that internal protocols exist for evaluating and managing donors, time frames for donation, and interactions with families, among other requirements. CMS does not, however, set out what those protocols should be. It also requires data on topics including deaths, organs that weren’t recovered, consent for donation, and number of donors.
The reality is we need to be held accountable to do our very best job.
Diane Brockmeier, Mid-America Transplant
The procurement organizations’ trade association, AOPO, previously conducted accreditation audits of the organizations that included greater specificity in some of these areas. It stopped in late 2021, the same year the new CMS performance standards were enacted.
The death notification registration is missing measures that would allow regulators to look more closely at soft skills that greatly affect the donation process. CMS, the nonprofits’ main regulator, already has mechanisms in other areas of its oversight that could capture this. Families of hospice patients, for example, are required to fill out a survey that asks if the hospice workers kept them updated about their loved one’s care, listened to them, attended to them in a timely fashion, and treated their loved one with respect, rating the hospice center on a scale of zero to 10.
Beyond that, six organ procurement organizations volunteered to open their books by sharing 10 years of such data with the Massachusetts Institute of Technology’s (MIT) Healthy ML Lab for analysis “to better understand where and how potential donors are lost, including by race and ethnicity,” according to the 2021 partnership announcement. The collaboration is still under way. McBride’s organization, OurLegacy, is one of the participating procurement organizations. LiveOnNY was previously part of the effort but has since withdrawn, McBride said.
The data shared with MIT includes a vast amount of information about the intricacies of the organizations’ performance, including the time their nonprofits showed up at the hospital, when they approached a family, the family’s response, and when they started allocating organs.
“Every decision we make, every action we take, is included in that database,” she said.
AOPO, Massa said, “supports data sharing.” It is currently working on a data-sharing effort with an outside consultant “with the goal of increasing donation and transplantation rates” that includes information on “referrals, patient demographics, authorization, and organs recovered and transplanted.” It is not mandatory.
Addressing these issues would require more transparency around this kind of organ procurement organization data and for regulators to use the data that is already collected.
“The reality is we need to be held accountable to do our very best job,” said Diane Brockmeier, CEO of Missouri-based procurement organization Mid-America Transplant. It ranked in the top performance tier. “Patients deserve that.”